Welcome to the world’s first comprehensive guide to CPL and associated conditions; for owners, veterinary professionals and complimentary therapists in the equine industry. We are CPL Awareness CIC – a non-profit company – and we aim to improve education and understanding of this complex disease. Our work is endorsed by veterinary and equine industry professionals across the world.
You can purchase digital Care Guides and Presentations from our BMAC shop here and all funds go to support the CIC.
What is CPL?
Chronic Progressive Lymphoedema is a disease affecting draft horses and cobs with feather. The lymphatic system fails, causing inflammation and fibrosis all four legs (although the hinds may appear first or worst affected). The horse will have hyperkeratosis, unrestricted to the typical areas and their lower legs will develop a cone-shape as the fill, thickening first at the fetlock/pastern and then further up the leg. There will be lumps, bumps and skin folds which deepen and harden as the disease progresses – that is the fibrosis. There may be round, penny-sized sores. Myasis as a result of maceration and exudate is common. CPL is so unique in it’s physical presentation that it can be diagnosed on that alone. Invasive procedures to diagnose are unhelpful, unnecessary and can be harmful and expensive.
CPL is a genetic disease with strong prevalence in family lines, therefore heritable (Brys, 2023). But the progression or “severity” of the disease itself can be broken down into the following percentages: –
14% influenced by the horse’s genetics
86% influenced by husbandry, environment, feed, parasites.
This gives owners and guardians 86% reasonable control over the progression of the disease – within their own means and limitations, of course.

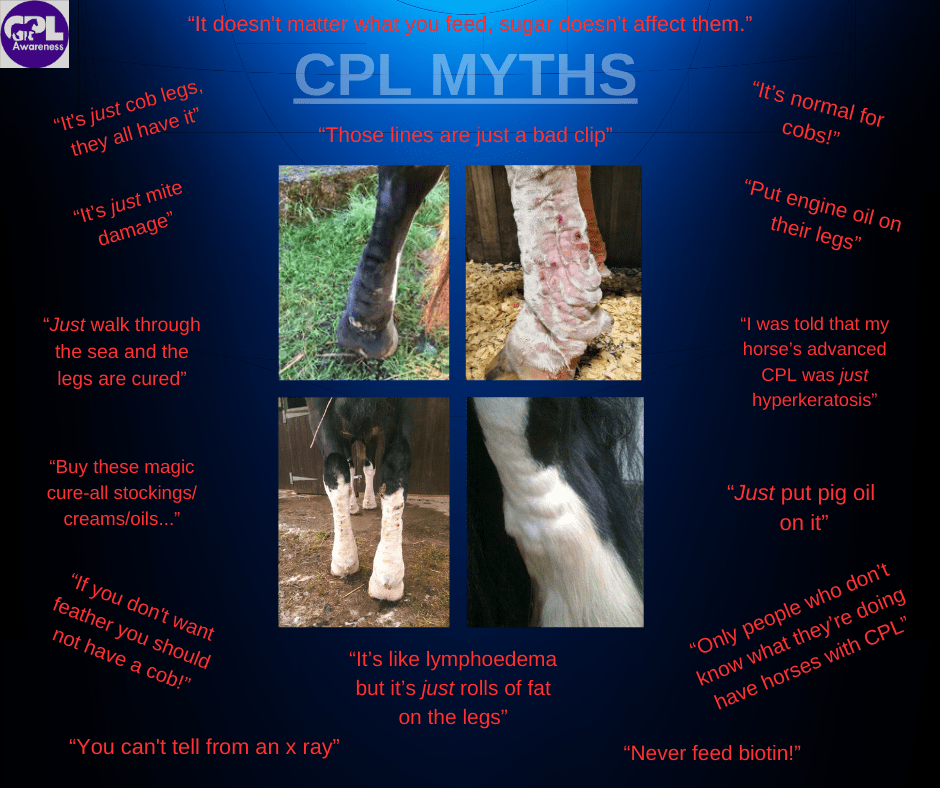
or myth? 2022
Horses may also exhibit the same presentation on their neck crests and docks. Increasingly I think we need to refer to CPL as a whole-horse disease.
CPL is frequently misdiagnosed as feather mites, “cob legs”, scarring and mud fever/greasy heel.
The disease affects Brabant (the traditional Belgian draft) horses at a prevalence of around 80>%. From experience I suspect that cobs/gypsy vanners are at a similar prevalence if not higher. Other breeds affected are: – Shires, Clydesdales, Friesians, Fells, all of the heavy, hairy European draft horses, some Percheron, Boulonnais, Welsh Section D, Poitou donkeys, mammoth donkeys.
These horses are also prone to chronic thrush which can appear to be treatment-resistant and they may also develop laminitis. It would be fair to say that many CPL horses live with a low-grade inflammation in the hooves.
CPL causes the legs to be immuno-compromised so the risk of secondary infection is higher.
It is important to note that feathered horses, especially with CPL, are prone to hyperkeratosis (an over-production of keratin) which causes skin crusts on which feather mites feed. Left untreated these mites can cause scarring and damage to the delicate tissue and superficial lymph vessels and as such must be recognised as one of the major triggers of CPL.
The major factors affecting CPL are as follows: –
Breed
Feather mites
Poor husbandry/hygiene
Inappropriate diet
Restriction of movement
Hyperkeratosis
Obesity
Secondary infection and intertrigo
CPL can be effectively managed and even reduced by addressing the disease holistically and following the CPL Management Protocol.
CPL can occur on it’s own or alongside another disease called Chronic Proliferative Pastern Dermatitis (CPPD), also known as “verrucous pastern dermatitis”. In the past the two have been confused in descriptions, but they are separate diseases. You will not see a horse with CPPD that doesnt also have CPL. CPPD has also been linked to feather mites.
“C.bovis infestation may affect the progression of chronic pastern dermatitis (also known as chronic proliferative pastern dermatitis, chronic progressive lymphoedema and dermatitis verrucosa) in draft horses, manifesting with oedema, lichenification and excessive skin folds that can progress to verruciform lesions.”
Silvia RüfenachtPetra J. RoosjeHeinz SagerMarcus G. DoherrReto StraubPamela Goldinger‐MüllerVincent Gerber




Not to be confused with Chronic Proliferative/verrucous Pastern Dermatitis.

Is this CPL?
In yellow is a crease caused by hyperkeratosis. It is essentially “mallenders“, just further down the leg. Once the area has been allowed to scar like that it can create problems for the superficial drainage as the lymph can not pass through scar tissue thicker than 4mm.
Creasing like this can be prevented to some degree by applying an emollient regularly and using something like Sebolytic® shampoo to remove the keratin build up and restore the natural balance of the skin.

We will see oedema start to develop around crease and gravity will bring that further down around the joint – see the minor folds developing, highlighted in red. Regardless of whether we think the horse will develop actual CPL, the best course of action is to treat as though it is, while also remembering to apply emollient to the area to prevent any further keratin build up and scarring. The area directly around the ergot may become puffy.
Below we can see two more unfortunate examples of this hyperkeratosis creasing and the subsequent oedema and loss of definition, as the leg starts to develop the familiar “traffic cone” shape and folds.




Thanks to the members of the CPL Facebook Group for submitting the above images.
